“Dr. Brian Jacob has extensive experience with hernia mesh removal and chronic pain treatment procedures in New York City.”
Dr. Jacob is regarded by peers as one of the top surgeons in the United States to help work-up, diagnose, and treat chronic pain in the groin and pelvis, including pain after hernia repairs or sports injuries.
We realize you have already probably spent months or years in search of a cure for your chronic pain. Dr. Jacob understands the significant frustration and suffering that may accompany this process, and will apply his deep level of understanding of the extensive list of possible causes of chronic pain to help you find your path to a cure.
Sometimes a hernia mesh, tack, or suture implant is related to the pain cause, but not always. The overwhelming majority of mesh, tack, and suture implants used to repair hernias do not cause any harm, pain, or injury. However, when these implants are related to the pain cause, it may be necessary to remove them. Remember, it is very important to recall if you have any abdominal pain, chronic groin pain, or leg pain BEFORE your hernia operation, if you had one. Oftentimes, the pain that patients experience after a hernia repair may have actually been existing BEFORE the hernia repair itself. This detail, as well as WHEN the pain actually started is very important to document. Patients must also remember that even after mesh, tacks, and sutures are removed, the pain may possibly continue, the pain may worsen or spread, and the hernia can also return. Mesh removal is unfortunately not a guaranteed cure for all chronic pain.
The best way to help patients resolve the pain is to understand the entire and thorough story behind the onset of the pain.
The Important Initial Consult with Dr. Jacob
Dr. Jacob will devote most of your initial office visit to listening, learning, and untangling your history and story surrounding your pain. This is NOT insurance-based care. Dr. Jacob provides a concierge-level of attunement and care that is absolutely necessary to begin to provide a solution for your pain. After the story is well understood, you will receive a detailed pain-focused examination, and then you will likely be sent for imaging that may include a sonogram, a CT scan, or an MRI. Once the imaging is complete, he will see you again to provide a definitive plan.

What People Say About Us!
"Caring and compassionate, sees his patients through to full recovery. Amazing and supportive through fear, questions and concerns.. Highly recommend."
Click here to read more reviews.
What is chronic pain?
The typical recovery after a laparoscopic inguinal hernia repair is associated with mild to moderate incisional pain and mild groin discomfort. This may last anywhere from 2 – 14 days, but is almost always gone by the 3rd or 4th week after surgery. The groin discomfort may be secondary to the gas used during surgery, the dissection, or rarely the mesh material or tacks (if used). There are a variety of mesh fixation materials that surgeons may choose to use, and all have a rare, but possible association with causing groin pain. These fixation options include (staples, permanent tacks, absorbable tacks, or glues). Some surgeons do repair without using mesh fixation materials at all.
Chronic pain is pain that has been present and consistent for at least 12 weeks.
Chronic Pain Surgical Treatment Options
- Hernia mesh removal
- Suture and surgical tack removal
- Recurrent hernia repairs
- Removal of lipoma
- Spermatic cord adhesiolysis
- Neurectomy (removal of nerves)
Chronic Pain Non-Surgical Treatment Options
Sometimes your chronic pain will not require a surgery as part of the treatment, and instead you may require:
- Physical therapy
- Oral medicines (nonsteroidals, antiinflamatory, or other pain reducing medications)
- Local office-based trigger spot injections
- Consult to a pain management specialist
- Consult to a mental health specialist
- Consults to alternative healing specialist
- Consult to another surgical specialist
Regardless of the diagnosis, Dr. Jacob will leave you with a confident and clear plan.
Acute Severe Groin Pain
Groin pain that is severe immediately after surgery should be brought to your surgeon’s attention, as this can be due to direct irritation from surgical material and could warrant return to the operating room to remove the foreign material or tack (if used). Fortunately, this risk is extremely rare. Should it occur, however, acute nerve injury could increase the risk of developing chronic pain.
Chronic Groin Pain
Chronic Groin Pain (can be mild or severe) is defined as the presence of pain, discomfort, or hypersensitivity (not present before surgery) existing for more than 3 months after surgery. According to one national database, even a healthy male with no previous history of groin pain has as high as a 6% risk of developing chronic discomfort after undergoing any type of inguinal hernia repair. While the general risks of developing this chronic discomfort exist, our group’s experience has kept this complication at an absolute minimum.
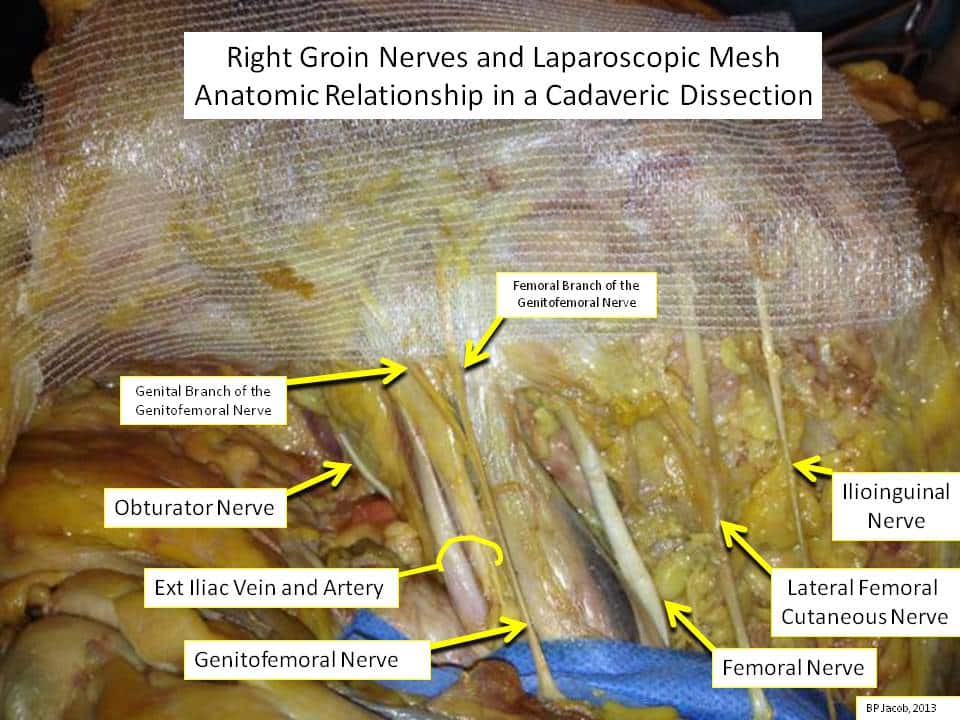
There are 6 nerves in the groin that your surgeon is aware of and will avoid harm to.
Lateral Femoral Cutaneous Nerve
This nerve is the most lateral nerve in the groin, innervates the upper lateral thigh skin, and in the past was the most common nerve irritated during a laparoscopic repair. If irritated, there may be pain or hypersensitivity experienced along the lateral thigh.
Genitofemoral (GF) Nerve
This nerve and its terminal branches are not routinely dissected out during a routine laparoscopic repair, but are well known to exist in the region just medial to the psoas muscle and lateral to the external iliac vein. The location of the two terminal branches varies. The trunk or either branch, however, can be potentially irritated or injured by the dissection, a tack, or by the mesh material. By limiting the use of tacks near its known location, injury to it can be minimized. The genital branch runs in the inguinal canal, under the spermatic cord in men and round ligament in women, and innervates the inner thigh and the lateral scrotal skin in men, and the labia majora in women. Its irritation is usually perceived by a hypersensitive scrotum in males and hypersensitive labia majora in females. The femoral branch innervates the anterior thigh, and irritation can lead to pain or hypersensitivity of the upper anterior thigh.
Femoral nerve
Like the GF nerve above, this nerve is not routinely identified during routine laparoscopic hernia dissection, but it does exist just lateral to the psoas muscle and entering the leg lateral to the femoral artery. Rather rarely, it at risk to be irritated or injured by use of a tack below the ileopubic tract. Even rarer, mesh can irritate this nerve. By limiting the use of tacks near its known location, injury to it can be minimized. If irritated or injured, leg muscles may feel heavy or weak, or pain along the leg may result.
Iliohypogastric Nerve
This nerve may only be injured during a laparoscopic repair if a tack were to penetrate through the muscle and into the nerve. The incidence of irritation during a laparoscopic repair is extremely rare. Pain or hypersensitivity to the suprapubic region or groin may occur.
Ilioinguinal Nerve
This nerve may be injured during a laparoscopic inguinal hernia repair only if your surgeon uses tacks and these tacks penetrate through muscle into this nerve. Its injury during a laparoscopic repair is extraordinarily rare. Irritation causes pain or hypersensitivity to the medial thigh, shaft of the penis, or groin.
Paravasal Nerve Fibers
Irritation of these may cause temporary testicular discomfort.
Any additional questions?
If you have any additional questions or would like to schedule an appointment with one of our trusted hernia repair specialists, call NYC Hernia™ today at 212-879-6677 or fill out the form below.